Buy Psilocybin (4-PO-DMT) Cas 520-52-5
Buy Psilocybin (4-PO-DMT) Cas 520-52-5
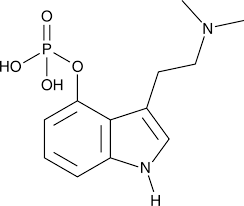
Psilocybin, also known as 4-phosphoryloxy-N,N-dimethyltryptamine (4-PO-DMT),[a] is a naturally occurring tryptamine alkaloid and investigational drug found in more than 200 species of mushrooms, with hallucinogenic and serotonergic effects.[20][25] Effects include euphoria, changes in perception, a distorted sense of time,[26] and perceived spiritual experiences. It can also cause adverse reactions such as nausea and panic attacks.[27]
Psilocybin is a prodrug of psilocin.[20] That is, the compound itself is biologically inactive but quickly converted by the body to psilocin.[20] Psilocybin is transformed into psilocin by dephosphorylation mediated via phosphatase enzymes.[28][20] Psilocin is chemically related to the neurotransmitter serotonin and acts as a non-selective agonist of the serotonin receptors.[20] Activation of one serotonin receptor, the serotonin 5-HT2A receptor, is specifically responsible for the hallucinogenic effects of psilocin and other serotonergic psychedelics.[20] Psilocybin is usually taken orally.[20] By this route, its onset is about 20 to 50 minutes, peak effects occur in about 1 to 2 hours, and its duration is about 4 to 6 hours.[11][19][20][14]
Psilocybin mushrooms were used ritualistically in pre-Columbian Mexico, but claims of their widespread ancient use are largely exaggerated and shaped by modern idealization and ideology.[29] In 1958, the Swiss chemist Albert Hofmann isolated psilocybin and psilocin from the mushroom Psilocybe mexicana. His employer, Sandoz, marketed and sold pure psilocybin to physicians and clinicians worldwide for use in psychedelic therapy. Increasingly restrictive drug laws of the 1960s and the 1970s curbed scientific research into the effects of psilocybin and other hallucinogens, but its popularity as an entheogen grew in the next decade, owing largely to the increased availability of information on how to cultivate psilocybin mushrooms.
Possession of psilocybin-containing mushrooms has been outlawed in most countries, and psilocybin has been classified as a Schedule I controlled substance under the 1971 United Nations Convention on Psychotropic Substances. Psilocybin is being studied as a possible medicine in the treatment of psychiatric disorders such as depression, substance use disorders, obsessive–compulsive disorder, and other conditions such as cluster headaches.[30] Psilocybin was approved for treatment-resistant depression in Australia in 2023.[31][32] It is in late-stage clinical trials in the United States for treatment-resistant depression.[33][34][35] A decision on approval of psilocybin for this indication is expected by the end of 2026.[36] Especially at higher doses and combined with psychological support, single doses of psilocybin can produce rapid and long-lasting antidepressant effects that generally outperform placebo, though they show only modest advantages over conventional continuous antidepressants like selective serotonin reuptake inhibitor (SSRIs); the quality of evidence is generally low and trial bias is common.[37][38][39][40][41]
Uses
Psilocybin is used recreationally, spiritually (as an entheogen), and medically.[42] It is primarily taken orally, but other routes of administration, such as intravenous injection, are sometimes employed by licensed medical researchers using pharmaceutical-grade psilocybin powder designed for injection. Injection should never be attempted by unlicensed people.[7]
Medical
In 2023, the Therapeutic Goods Administration (TGA) approved psilocybin for treatment of treatment-resistant depression in Australia.[43][44][45] It is also under development for the treatment of depression and for various other indications elsewhere, such as the United States and Europe, but has not yet been approved in other countries (see below).[10][30][35]
Dosing
Psilocybin is used as a psychedelic at doses of 5 to 40 mg orally.[14][46] Low doses are 5 to 10 mg, an intermediate or “good effect” dose is 20 mg, and high or ego-dissolution doses are 30 to 40 mg.[14][46] Psilocybin’s effects can be subjectively perceived at a dose as low as 3 mg per 70 kg body weight.[46][47] Microdosing involves the use of subthreshold psilocybin doses of less than 2.5 mg.[14][46]
When psilocybin is used in the form of psilocybin-containing mushrooms, microdoses are 0.1 g to 0.3 g and psychedelic doses are 1.0 g to 3.5–5.0 g in the case of dried mushrooms.[48][49][7] The preceding 1.0 to 5.0 g range corresponds to psilocybin doses of about 10 to 50 mg.[7] Psilocybin-containing mushrooms vary in their psilocybin and psilocin content, but are typically around 1% of the dried weight of the mushrooms (in terms of total or combined psilocybin and psilocin content).[49][50][21][7][28][51][52][53] Psilocin is about 1.4 times as potent as psilocybin because of the two compounds’ difference in molecular weight.[21][54][55]
“Lemon tek” or “lemon tekking” is a method sometimes used by recreational psilocybin users.[56][57][58] It involves soaking psilocybin-containing mushrooms in citric acid-containing lemon juice to supposedly convert their psilocybin content into psilocin before administration.[56][57][58] This is claimed to hasten their onset, cause a sharper and more intense peak, and shorten their duration.[56][57][58]
Available forms
Psilocybin is most commonly consumed in the form of psilocybin-containing mushrooms, such as Psilocybe species like Psilocybe cubensis. It may also be prepared synthetically, but outside of research settings it is not typically used in this form. Regardless of form, psilocybin is usually taken orally. The psilocybin present in certain species of mushrooms can be ingested in several ways: by consuming fresh or dried fruit bodies, by preparing an herbal tea, or by combining with other foods to mask the bitter taste.[59] In rare cases people have intravenously injected mushroom extracts, with serious medical complications such as systemic mycological infection and hospitalization.[60][61][62][63] Another form of psilocybin (as well as of related psychedelics like 4-AcO-DMT) is mushroom edibles such as chocolate bars and gummies, which may be purchased at psychedelic mushroom stores.
Effects

Psilocybin produces a variety of psychological, perceptual, interpersonal, and physical effects.[14]
Psychological and perceptual effects

After ingesting psilocybin, the user may experience a wide range of emotional effects, which can include disorientation, lethargy, giddiness, euphoria, joy, and depression. In one study, 31% of volunteers given a high dose reported feelings of significant fear and 17% experienced transient paranoia.[60] In studies at Johns Hopkins University, among those given a moderate dose (but enough to “give a high probability of a profound and beneficial experience”), negative experiences were rare, whereas one-third of those given a high dose experienced anxiety or paranoia.[64][65] Low doses can induce hallucinatory effects. Closed-eye hallucinations may occur, where the affected person sees multicolored geometric shapes and vivid imaginative sequences.[47] Some people report synesthesia, such as tactile sensations when viewing colors.[66]: 175 At higher doses, psilocybin can lead to “intensification of affective responses, enhanced ability for introspection, regression to primitive and childlike thinking, and activation of vivid memory traces with pronounced emotional undertones”.[67] Open-eye visual hallucinations are common and may be very detailed, although rarely confused with reality.[47]
Psilocybin is known to strongly affect the subjective experience of the passage of time.[68][26] Users often feel as if time is slowed down, resulting in the perception that “minutes appear to be hours” or “time is standing still”.[69] Studies have demonstrated that psilocybin significantly impairs subjects’ ability to gauge time intervals longer than 2.5 seconds, impairs their ability to synchronize to inter-beat intervals longer than 2 seconds, and reduces their preferred tapping rate.[69][70] These results are consistent with the drug’s role in affecting prefrontal cortex activity[71] and the role that the prefrontal cortex plays in time perception,[72] but the neurochemical basis of psilocybin’s effects on perception of time is not known with certainty.[73]
Users having a pleasant experience can feel a sense of connection to others, nature, and the universe; other perceptions and emotions are also often intensified. Users having an unpleasant experience (a “bad trip“) describe a reaction accompanied by fear, other unpleasant feelings, and occasionally by dangerous behavior. The term “bad trip” is generally used to describe a reaction characterized primarily by fear or other unpleasant emotions, not just a transitory experience of such feelings. A variety of factors may contribute to a bad trip, including “tripping” during an emotional or physical low or in a non-supportive environment (see: set and setting). Ingesting psilocybin in combination with other drugs, including alcohol, can also increase the likelihood of a bad trip.[60][74] Other than the duration of the experience, the effects of psilocybin are similar to comparable doses of lysergic acid diethylamide (LSD) or mescaline. But in the Psychedelics Encyclopedia, author Peter Stafford writes: “The psilocybin experience seems to be warmer, not as forceful and less isolating. It tends to build connections between people, who are generally much more in communication than when they use LSD.”[75]: 273
Set and setting and moderating factors
The effects of psilocybin are highly variable and depend on the mindset and environment in which the user has the experience, factors commonly called set and setting. In the early 1960s, Timothy Leary and his Harvard colleagues investigated the role of set and setting in psilocybin’s effects. They administered the drug to 175 volunteers (from various backgrounds) in an environment intended to be similar to a comfortable living room. 98 of the subjects were given questionnaires to assess their experiences and the contribution of background and situational factors. Those who had prior experience with psilocybin reported more pleasant experiences than those for whom the drug was novel. Group size, dose, preparation, and expectancy were important determinants of the drug response. In general, those in groups of more than eight felt that the groups were less supportive and their experiences less pleasant. Conversely, smaller groups (fewer than six) were seen as more supportive and reported more positive reactions to the drug in those groups. Leary and colleagues proposed that psilocybin heightens suggestibility, making a user more receptive to interpersonal interactions and environmental stimuli.[76] These findings were affirmed in a later review by Jos ten Berge (1999), who concluded that dose, set, and setting are fundamental factors in determining the outcome of experiments that tested the effects of psychedelic drugs on artists’ creativity.[77]
Further studies demonstrate that supportive settings significantly reduce the likelihood of adverse reactions, including panic, paranoia, or psychological distress. Positive therapeutic outcomes are strongly correlated with the participant’s trust in the environment and the facilitators.[78][79]
Theory of mind network and default mode network
Psychedelics, including psilocybin, have been shown to affect different clusters of brain regions known as the “theory of mind network” (ToMN) and the default mode network (DMN).[80] The ToMN involves making inferences and understanding social situations based on patterns,[81] whereas the DMN relates more to introspection and one’s sense of self.[80] The DMN, in particular, is related to increased rumination and worsening self-image in patients with major depressive disorder (MDD).[82] In studies done with single use psilocybin, areas of the DMN showed decreased functional connectivity (communication between areas of the brain). This provides functional insight into the work of psilocybin in increasing one’s sense of connection to one’s surroundings, as the areas of the brain involved in introspection decrease in functionality under the effects of the drug.[83] Conversely, areas of the brain involved in the ToMN showed increased activity and functional activation in response to psychedelics. These results were not unique to psilocybin and there was no significant difference in brain activation found in similar trials of mescaline and LSD. Information and studies into the DMN and ToMN are relatively sparse and their connections to other psychiatric illnesses and the use of psychedelics is still largely unknown.[80]
Group perceptions
Through further anthropological studies regarding “personal insights”[84] and the psychosocial effects of psilocybin, it can be seen in many traditional societies that powerful mind-active substances such as psilocybin are regularly “consumed ritually for therapeutic purposes or for transcending normal, everyday reality”.[85] Positive effects that psilocybin has on individuals can be observed by taking on an anthropological approach and moving away from the Western biomedical view; this is aided by the studies done by Leary.[86] Within certain traditional societies, where the use of psilocybin is frequent for shamanic healing rituals, group collectives praise their guide, healer and shaman for helping alleviate their pains, aches and hurt. They do this through a group ritual practice where the group, or just the guide, ingests psilocybin to help extract any “toxic psychic residues or sorcerous implants”[85] found in one’s body.
Group therapies using “classic” psychedelics are becoming more common within clinical practice in the Western world.[87] This is speculated to grow, provided the evidence remains indicative of their safety and efficacy.[88] In social sense, the group is shaped by their experiences surrounding psilocybin and how they view the fungus collectively. As mentioned in the anthropology article,[85] the group partakes in a “journey” together, thus adding to the spiritual, social body where roles, hierarchies and gender are subjectively understood.[85]
Cultural significance and “mystical” experiences

Psilocybin mushrooms have been and continue to be used in Indigenous American cultures in religious, divinatory, or spiritual contexts. Reflecting the meaning of the word entheogen (“the god within”), the mushrooms are revered as powerful spiritual sacraments that provide access to sacred worlds. Typically used in small group community settings, they enhance group cohesion and reaffirm traditional values.[89] Terence McKenna documented the worldwide practices of psilocybin mushroom usage as part of a cultural ethos relating to the Earth and mysteries of nature, and suggested that mushrooms enhanced self-awareness and a sense of contact with a “Transcendent Other”—reflecting a deeper understanding of our connectedness with nature.[90]
Psychedelic drugs can induce states of consciousness that have lasting personal meaning and spiritual significance in religious or spiritually inclined people; these states are called mystical experiences. Some scholars have proposed that many of the qualities of a drug-induced mystical experience are indistinguishable from mystical experiences achieved through non-drug techniques such as meditation or holotropic breathwork.[91][92] In the 1960s, Walter Pahnke and colleagues systematically evaluated mystical experiences (which they called “mystical consciousness”) by categorizing their common features. According to Pahnke, these categories “describe the core of a universal psychological experience, free from culturally determined philosophical or theological interpretations”, and allow researchers to assess mystical experiences on a qualitative, numerical scale.[93]
In the 1962 Marsh Chapel Experiment, run by Pahnke at the Harvard Divinity School under Leary’s supervision,[94] almost all the graduate degree divinity student volunteers who received psilocybin reported profound religious experiences.[95] One of the participants was religious scholar Huston Smith, author of several textbooks on comparative religion; he called his experience “the most powerful cosmic homecoming I have ever experienced.”[96] In a 25-year followup to the experiment, all the subjects given psilocybin said their experience had elements of “a genuine mystical nature and characterized it as one of the high points of their spiritual life”.[97]: 13 Psychedelic researcher Rick Doblin considered the study partially flawed due to incorrect implementation of the double-blind procedure and several imprecise questions in the mystical experience questionnaire. Nevertheless, he said that the study cast “considerable doubt on the assertion that mystical experiences catalyzed by drugs are in any way inferior to non-drug mystical experiences in both their immediate content and long-term effects”.[97]: 24 Psychiatrist William A. Richards echoed this sentiment, writing in a 2007 review, “[psychedelic] mushroom use may constitute one technology for evoking revelatory experiences that are similar, if not identical, to those that occur through so-called spontaneous alterations of brain chemistry.”[98]
A group of researchers from Johns Hopkins School of Medicine led by Roland Griffiths conducted a study to assess the immediate and long-term psychological effects of the psilocybin experience, using a modified version of the mystical experience questionnaire and a rigorous double-blind procedure.[99] When asked in an interview about the similarity of his work to Leary’s, Griffiths explained the difference: “We are conducting rigorous, systematic research with psilocybin under carefully monitored conditions, a route which Dr. Leary abandoned in the early 1960s.”[100] Experts have praised the National Institute of Drug Abuse-funded study, published in 2006, for the soundness of its experimental design.[b] In the experiment, 36 volunteers with no experience with hallucinogens were given psilocybin and methylphenidate (Ritalin) in separate sessions; the methylphenidate sessions served as a control and psychoactive placebo. The degree of mystical experience was measured using a questionnaire developed by Ralph W. Hood;[101] 61% of subjects reported a “complete mystical experience” after their psilocybin session, while only 13% reported such an outcome after their experience with methylphenidate. Two months after taking psilocybin, 79% of the participants reported moderately to greatly increased life satisfaction and sense of well-being. About 36% of participants also had a strong to extreme “experience of fear” or dysphoria (i.e., a “bad trip”) at some point during the psilocybin session (which was not reported by any subject during the methylphenidate session); about one-third of these (13% of the total) reported that this dysphoria dominated the entire session. These negative effects were reported to be easily managed by the researchers and did not have a lasting negative effect on the subject’s sense of well-being.[102]
A follow-up study 14 months later confirmed that participants continued to attribute deep personal meaning to the experience. Almost a third of the subjects reported that the experience was the single most meaningful or spiritually significant event of their lives, and over two-thirds reported it was among their five most spiritually significant events. About two-thirds said the experience increased their sense of well-being or life satisfaction.[95] Even after 14 months, those who reported mystical experiences scored on average 4 percentage points higher on the personality trait of Openness/Intellect; personality traits are normally stable across the lifespan for adults. Likewise, in a 2010 web-based questionnaire study designed to investigate user perceptions of the benefits and harms of hallucinogenic drug use, 60% of the 503 psilocybin users reported that their use of psilocybin had a long-term positive impact on their sense of well-being.[60][103]
Physical effects
Common responses include pupil dilation (93%); changes in heart rate (100%), including increases (56%), decreases (13%), and variable responses (31%); changes in blood pressure (84%), including hypotension (34%), hypertension (28%), and general instability (22%); changes in stretch reflex (86%), including increases (80%) and decreases (6%); nausea (44%); tremor (25%); and dysmetria (16%) (inability to properly direct or limit motions).[2][c] Psilocybin’s sympathomimetic or cardiovascular effects, including increased heart rate and blood pressure, are usually mild.[42][2] On average, peak heart rate is increased by 5 bpm, peak systolic blood pressure by 10 to 15 mm Hg, and peak diastolic blood pressure by 5 to 10 mm Hg.[42][2] But temporary increases in blood pressure can be a risk factor for users with preexisting hypertension.[47] Psilocybin’s somatic effects have been corroborated by several early clinical studies.[105] A 2005 magazine survey of clubgoers in the UK found that over a quarter of those who had used psilocybin mushrooms in the preceding year experienced nausea or vomiting, although this was caused by the mushroom rather than psilocybin itself.[60] In one study, administration of gradually increasing doses of psilocybin daily for 21 days had no measurable effect on electrolyte levels, blood sugar levels, or liver toxicity tests.[2]
Onset and duration
The onset of action of psilocybin taken orally is 0.5 to 0.8 hours (30–50 minutes) on average, with a range of 0.1 to 1.5 hours (5–90 minutes).[14][11] Peak psychoactive effects occur at about 1.0 to 2.2 hours (60–130 minutes).[11][14] The time to offset of psilocybin orally is about 6 to 7 hours on average.[106] The duration of action of psilocybin is about 4 to 6 hours (range 3–12 hours) orally.[11][14][19] A small dose of 1 mg by intravenous injection had a duration of 15 to 30 minutes.[2][12] In another study, 2 mg psilocybin by intravenous injection given over 60 seconds had an immediate onset, reached a sustained peak after 4 minutes, and subsided completely after 45 to 60 minutes.[15][16]
Contraindications
Contraindications of psilocybin are mostly psychiatric conditions that increase the risk of psychological distress, including the rare adverse effect of psychosis during or after the psychedelic experience.[11][107] These conditions may include history of psychosis, schizophrenia, bipolar disorder, or borderline personality disorder.[11][108] Further research may provide more safety information about the use of psilocybin in people with such conditions.[11] It is notable in this regard that psilocybin and other psychedelics are being studied for the potential treatment of all the preceding conditions.[109][110][111][112][113][114] In the case of bipolar disorder, there are concerns that psychedelics may trigger a switch into mania.[115]
Psilocybin is considered to be contraindicated in women who are pregnant or breastfeeding due to insufficient research in this population.[11] There are transient increases in heart rate and blood pressure with psilocybin, and hence uncontrolled cardiovascular conditions are a relative contraindication for psilocybin.[11]
Serotonin 5-HT2A receptor antagonists such as atypical antipsychotics and certain antidepressants may block psilocybin’s hallucinogenic effects and hence may be considered contraindicated in this sense.[116][117] Monoamine oxidase inhibitors (MAOIs) may potentiate psilocybin’s effects and augment its risks.[116]
Adverse effects
Most of the comparatively few fatal incidents associated with psychedelic mushroom usage involve the simultaneous use of other drugs, especially alcohol. A common adverse effect resulting from psilocybin mushroom use involves “bad trips” or panic reactions, in which people become anxious, confused, agitated, or disoriented.[118] Accidents, self-injury, or suicide attempts can result from serious cases of acute psychotic episodes.[60] No studies have linked psilocybin with birth defects,[119] but it is recommended that pregnant women avoid its usage.[120]
Psychiatric adverse effects
Panic reactions can occur after consumption of psilocybin-containing mushrooms, especially if the ingestion is accidental or otherwise unexpected. Reactions characterized by violent behavior, suicidal thoughts,[121] schizophrenia-like psychosis,[122][123] and convulsions[124] have been reported in the literature. A 2005 survey conducted in the United Kingdom found that almost a quarter of those who had used psilocybin mushrooms in the past year had experienced a panic attack.[60] [failed verification] Less frequently reported adverse effects include paranoia, confusion, prolonged derealization (disconnection from reality), and mania.[103] Psilocybin usage can temporarily induce a state of depersonalization disorder.[125] Usage by those with schizophrenia can induce acute psychotic states requiring hospitalization.[126]
The similarity of psilocybin-induced symptoms to those of schizophrenia has made the drug a useful research tool in behavioral and neuroimaging studies of schizophrenia.[127][128][129] In both cases, psychotic symptoms are thought to arise from a “deficient gating of sensory and cognitive information” in the brain that leads to “cognitive fragmentation and psychosis”.[128] Flashbacks (spontaneous recurrences of a previous psilocybin experience) can occur long after psilocybin use. Hallucinogen persisting perception disorder (HPPD) is characterized by a continual presence of visual disturbances similar to those generated by psychedelic substances. Neither flashbacks nor HPPD are commonly associated with psilocybin usage,[60] and correlations between HPPD and psychedelics are further obscured by polydrug use and other variables.[130]
Tolerance and dependence

Tolerance to psilocybin builds and dissipates quickly; ingesting it more than about once a week can lead to diminished effects. Tolerance dissipates after a few days, so doses can be spaced several days apart to avoid the effect.[6] A cross-tolerance can develop between psilocybin and LSD,[132] and between psilocybin and phenethylamines such as mescaline and DOM.[133]
Repeated use of psilocybin does not lead to physical dependence.[2] A 2008 study concluded that, based on U.S. data from 2000 to 2002, adolescent-onset (defined here as ages 11–17) usage of hallucinogenic drugs (including psilocybin) did not increase the risk of drug dependence in adulthood; this was in contrast to adolescent usage of cannabis, cocaine, inhalants, anxiolytic medicines, and stimulants, all of which were associated with “an excess risk of developing clinical features associated with drug dependence”.[3] Likewise, a 2010 Dutch study ranked the relative harm of psilocybin mushrooms compared to a selection of 19 recreational drugs, including alcohol, cannabis, cocaine, ecstasy, heroin, and tobacco. Psilocybin mushrooms were ranked as the illicit drug with the lowest harm,[4] corroborating conclusions reached earlier by expert groups in the United Kingdom.[5]
Long-term effects
A potential risk of frequent repeated use of psilocybin and other psychedelics is cardiac fibrosis and valvulopathy caused by serotonin 5-HT2B receptor activation.[134][135] But single high doses or widely spaced doses (e.g., months apart) are thought to be safe, and concerns about cardiac toxicity apply more to chronic psychedelic microdosing or very frequent intermittent use (e.g., weekly).[134][135]
Overdose
Psilocybin has low toxicity, meaning that it has a low risk of inducing life-threatening events like breathing or heart problems.[136][118] Research shows that health risks may develop with use of psilocybin. Nonetheless, hospitalizations from it are rare, and overdoses are generally mild and self-limiting.[136][118] The lethal dose of psilocybin in humans is unknown, but has been estimated to be approximately 200 times a typical recreational dose.[136]
A review of the management of psychedelic overdoses suggested that psilocybin-related overdose management should prioritize managing the immediate adverse effects, such as anxiety and paranoia, rather than specific pharmacological interventions, as psilocybin’s physiological toxicity tends to be rather limited.[137] One analysis of people hospitalized for psilocybin poisoning found high urine concentrations of phenethylamine (PEA), suggesting that PEA might contribute to the effects of psilocybin poisoning.[137]
Despite acting as non-selective serotonin receptor agonists, psilocybin and other major serotonergic psychedelics like lysergic acid diethylamide (LSD) do not cause serotonin syndrome even in the context of extreme overdose.[138][136][139] This is thought to be because they act as partial agonists of serotonin receptors like the serotonin 5-HT2A receptor, in contrast to serotonin itself, which is a full agonist.[138][139]
In rats, the median lethal dose (LD50) of psilocybin when administered orally is 280 mg/kg, approximately 1.5 times that of caffeine. The lethal dose of psilocybin when administered intravenously in mice is 285 mg/kg, in rats is 280 mg/kg, and in rabbits is 12.5 mg/kg.[23][140] Psilocybin comprises approximately 1% of the weight of Psilocybe cubensis mushrooms, and so nearly 1.7 kilograms (3.7 lb) of dried mushrooms, or 17 kilograms (37 lb) of fresh mushrooms, would be required for a 60-kilogram (130 lb) person to reach the 280 mg/kg LD50 value of rats.[60] Based on the results of animal studies and limited human case reports, the human lethal dose of psilocybin has been extrapolated to be 2,000 to 6,000 mg, which is around 1,000 times greater than its effective dose of 6 mg and 200 times the typical recreational dose of 10 to 30 mg.[141][136] The Registry of Toxic Effects of Chemical Substances assigns psilocybin a relatively high therapeutic index of 641 (higher values correspond to a better safety profile); for comparison, the therapeutic indices of aspirin and nicotine are 199 and 21, respectively.[142] The lethal dose from psilocybin toxicity alone is unknown, and has rarely been documented—as of 2011, only two cases attributed to overdosing on hallucinogenic mushrooms (without concurrent use of other drugs) have been reported in the scientific literature, and those may involve factors other than psilocybin.[60][d]
Interactions
Serotonin 5-HT2A receptor antagonists can block the hallucinogenic effects of serotonergic psychedelics like psilocybin.[116][145] Numerous drugs act as serotonin 5-HT2A receptor antagonists, including antidepressants like trazodone and mirtazapine, antipsychotics like quetiapine, olanzapine, and risperidone, and other agents like ketanserin, pimavanserin, cyproheptadine, and pizotifen.[116][117] Such drugs are sometimes called “trip killers” because they can prevent or abort psychedelics’ hallucinogenic effects.[146][117][147] Serotonin 5-HT2A receptor antagonists that have been specifically shown in clinical studies to diminish or abolish psilocybin’s effects include ketanserin, risperidone, and chlorpromazine.[116][145]
The serotonin 5-HT1A receptor partial agonist buspirone has been found to markedly reduce psilocybin’s hallucinogenic effects in humans.[116][145][148][149] Conversely, the serotonin 5-HT1A receptor antagonist pindolol has been found to potentiate the hallucinogenic effects of the related psychedelic dimethyltryptamine (DMT) by 2- to 3-fold in humans.[149][150] Selective serotonin reuptake inhibitors (SSRIs) may modify psilocybin’s effects.[116][145][151] One clinical trial found that psilocybin’s hallucinogenic and “good drug” effects were not modified by the SSRI escitalopram, but that its “bad drug effects” such as anxiety, as well as ego dissolution, were reduced, among other changes.[145][116][151]
Benzodiazepines such as diazepam, alprazolam, clonazepam, and lorazepam, as well as alcohol, which act as GABAA receptor positive allosteric modulators, have been limitedly studied in combination with psilocybin and other psychedelics and are not known to directly interact with them.[145][116] But these GABAergic drugs produce effects such as anxiolysis, sedation, and amnesia, and may therefore diminish or otherwise oppose psychedelics’ effects.[116][146][117][147][152] Because of this, recreational users often use benzodiazepines and alcohol as “trip killers” to manage difficult hallucinogenic experiences with psychedelics, such as experiences with prominent anxiety.[146][117][147] This strategy’s safety is not entirely clear and might have risks,[146][145][117][147] but benzodiazepines have been used to manage psychedelics’ adverse psychological effects in clinical studies and in Emergency Rooms.[145][153][154][155][156] A clinical trial of psilocybin and midazolam coadministration found that midazolam clouded psilocybin’s effects and impaired memory of the experience.[157][158] Benzodiazepines might interfere with the therapeutic effects of psychedelics like psilocybin, such as sustained antidepressant effects.[159][160]
Psilocin, the active form of psilocybin, is a substrate of the monoamine oxidase (MAO) enzyme MAO-A.[161][106][21] The exact extent to which psilocin (and by extension psilocybin) is metabolized by MAO-A is not fully clear, but has ranged from 4% to 33% in different studies based on metabolite excretion.[161][106][21] Circulating levels of psilocin’s deaminated metabolite are far higher than those of free unmetabolized psilocin with psilocybin administration.[10][12] Combination of MAO-substrate psychedelics with monoamine oxidase inhibitors (MAOIs) can result in overdose and toxicity.[116] Examples of MAOIs that may potentiate psychedelics behaving as MAO-A substrates, such as psilocin, include phenelzine, tranylcypromine, isocarboxazid, and moclobemide, as well as harmala alkaloids like harmine and harmaline and chronic tobacco smoking.[116][162] An early clinical study of psilocybin in combination with short-term tranylcypromine pretreatment found that tranylcypromine marginally potentiated psilocybin’s peripheral effects, including pressor effects and mydriasis, but overall did not significantly modify its psychoactive and hallucinogenic effects, although some of its emotional effects were said to be reduced and some of its perceptual effects were said to be amplified.[42][163][164]
Psilocin may be metabolized to a minor extent by the cytochrome P450 (CYP450) enzymes CYP2D6 and/or CYP3A4 and appears unlikely to be metabolized by other CYP450 enzymes.[161][42] The role of CYP450 enzymes in psilocin’s metabolism seems to be small, and so considerable drug interactions with CYP450 inhibitors and/or inducers may not be expected.[161][42] Psilocin’s major metabolic pathway is glucuronidation by UDP-glucuronosyltransferase enzymes including UGT1A10 and UGT1A9.[145] Diclofenac and probenecid are inhibitors of these enzymes that theoretically might inhibit the metabolism of and thereby potentiate psilocybin’s effects,[145] but no clinical research or evidence on this possible interaction exists.[145] Few other drugs are known to influence UGT1A10 or UGT1A9 function.[145]

Reviews
There are no reviews yet.